
I have been impressed by the absolute support of the Glaucoma Community on Facebook. Specifically, the Living with Glaucoma Support Group has been very supportive of the community, with members offering help to others suffering from glaucoma. I have noticed there is a frequent question about when to give eye drops and why the timing matters. In short, each drop has a different effective time in the eye so some are given more frequently, and some are daily. Because there are peak times of eye fluid production in the eye, the eye drops are given to coincide with the natural rhythm of eye fluid production. Eye drops work best when you use them the right way and at consistent times.
Why Glaucoma Drops Are Prescribed
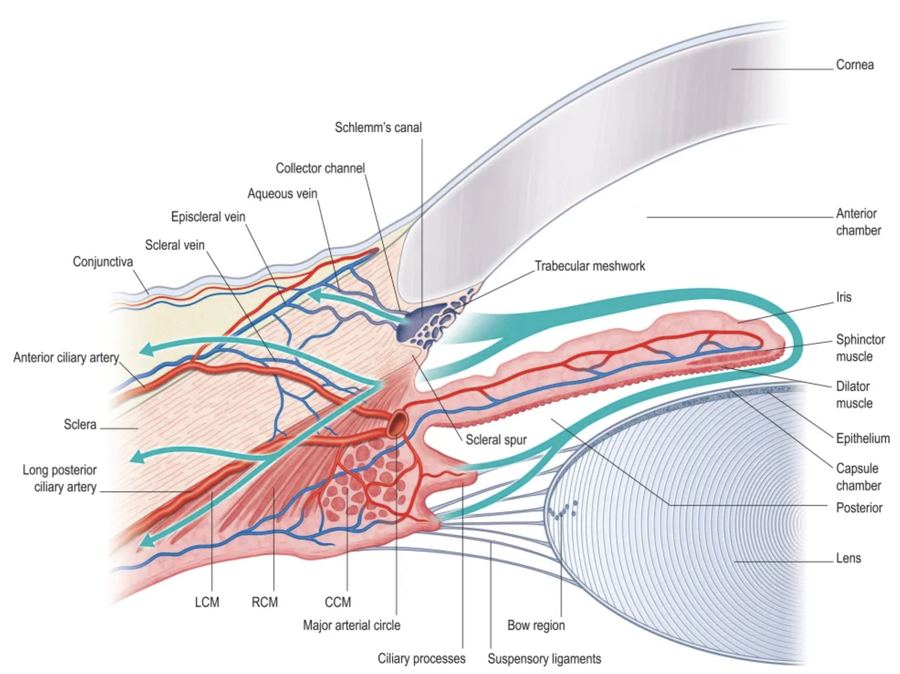
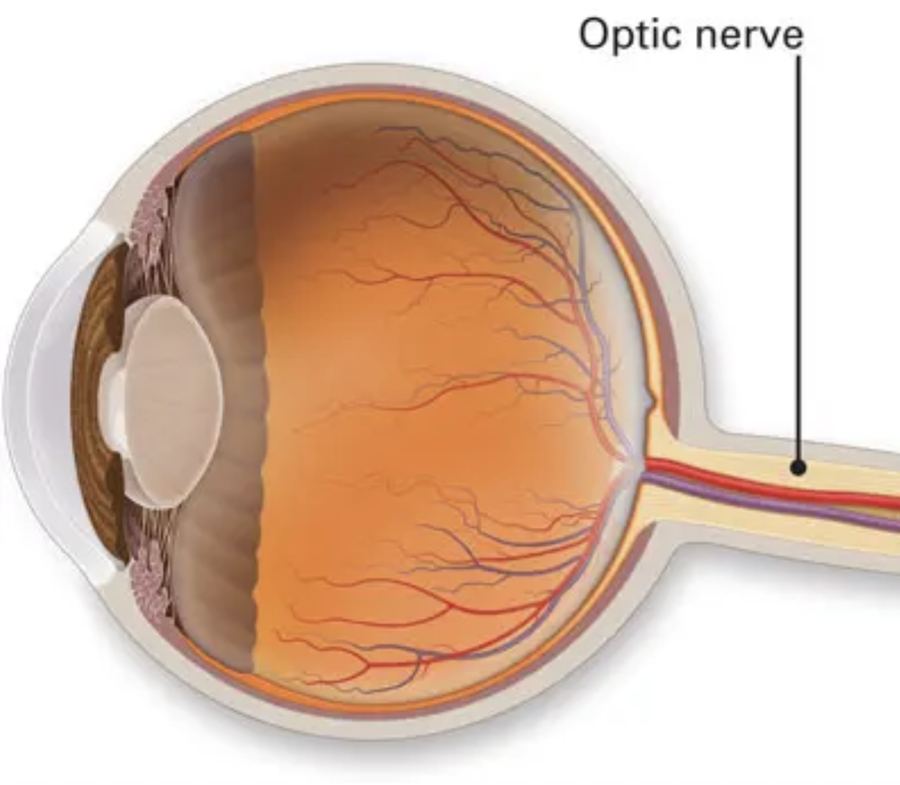
Inside your eye, a clear fluid is constantly being made and drained. If the eye makes too much fluid or the drain doesn't work well, pressure can build up, like a sink that's slowly clogging. Glaucoma drops help by making less fluid, helping fluid drain out better, or both (some combination drops do both). Lower, steadier eye pressure helps protect the optic nerve (the "cable" that carries vision to the brain).
Why Time of Day Matters: Your Eye Has a Daily Rhythm
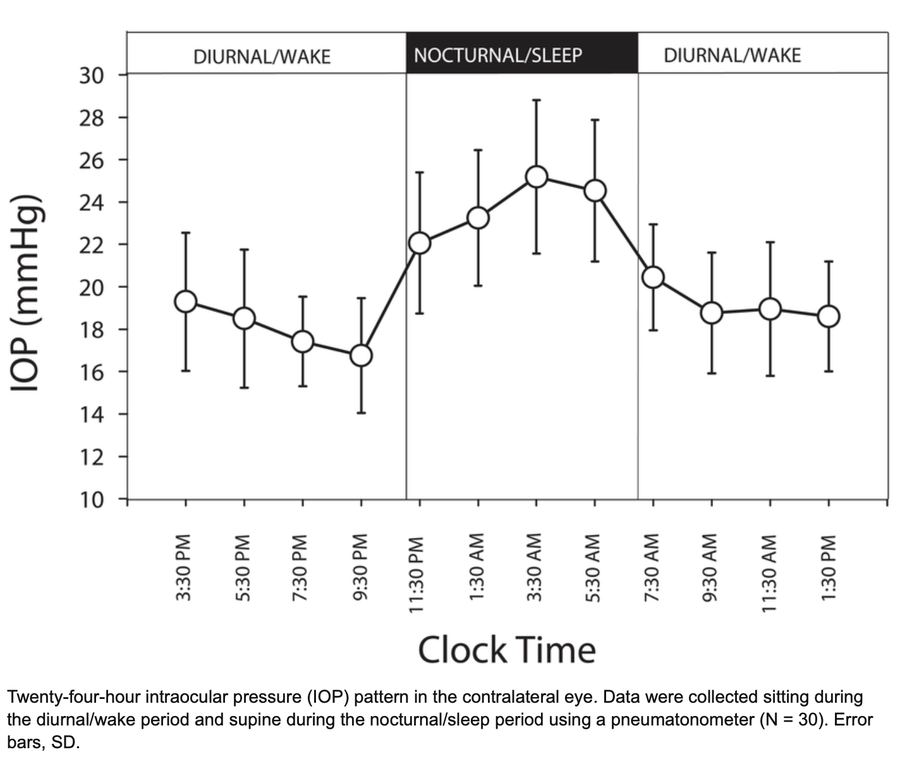
Your eye doesn't behave the same at 10 AM and 2 AM. Fluid production follows a body clock and tends to be higher during the day/morning and lower at night. Many people experience a classic early-morning pressure rise (often around the time you wake up), and some people have their highest pressures during the sleeping hours or early morning. So the time of day (or timing relative to your sleep cycle) is very important when you place your eye drops. That's one reason your doctor may care not just about your "office pressure," but also about coverage across the full 24 hours.
The Right Way to Put in Glaucoma Drops (Step-by-Step)
Wash your hands. Tilt your head back and look up. Pull down the lower lid to make a small "pocket." Put ONE drop in (more than one usually just spills out). Close your eye gently (don't squeeze hard). Press the inner corner of the eye (near the nose) for 2-3 minutes — this is called punctal occlusion and helps keep the medication in the eye and out of your throat/bloodstream. If you use more than one drop, wait at least 5 minutes between different bottles so the second drop doesn't wash out the first. Don't let the bottle tip touch your eye, lashes, or fingers.

Common Glaucoma Drop Types and Usual Dosing Schedule
Prostaglandin analogs (increase drainage) — examples: latanoprost, travoprost, bimatoprost, tafluprost (Xalatan, Travatan, Lumigan, Zioptan). Typical frequency: once daily. Ideal time: night/bedtime. Their strongest pressure-lowering effect lines up well with the "early morning" pressure rise. With latanoprost, eye pressure typically starts to drop a few hours after dosing, and the maximum effect is usually about 8-12 hours later — meaning if you use it at bedtime (say 10 PM), the strongest part of the effect often lands around early morning (roughly 6-10 AM), helping blunt the common early-morning/overnight pressure peak.
Beta blockers (reduce fluid production) — examples: timolol, betaxolol. Typical frequency: usually twice daily (sometimes once daily depending on formulation). Ideal time: morning (and late afternoon/early evening if twice daily). Fluid production is already lower during sleep, and beta blockers may have less nocturnal effect for many patients, so they're often more useful for daytime coverage.
Alpha agonists (reduce fluid + increase some drainage) — example: brimonidine. Typical frequency: 2-3 times per day, evenly spaced while awake. These tend to wear off faster, so spacing doses helps avoid "gaps" that can allow pressure to climb.
Carbonic anhydrase inhibitors (CAIs) (reduce fluid production) — examples: dorzolamide, brinzolamide (found in Azopt and Cosopt). Typical frequency: 2-3 times per day, evenly spaced while awake. Like beta blockers, they target fluid production, which naturally changes over 24 hours, so consistent dosing helps smooth out the pressure curve.
Rho-kinase inhibitor (increase drainage) — example: netarsudil (found in Rhopressa and Rocklatan). Typical frequency: once daily, at night/bedtime. The once-daily schedule supports adherence, and many clinicians place once-daily drops at night to help cover the early-morning rise.
Combination drops (two medicines in one bottle) — dorzolamide/timolol (Cosopt): twice daily. Brimonidine/timolol (Combigan): twice daily. Brinzolamide/brimonidine (Simbrinza): often three times daily. Netarsudil/latanoprost (Rocklatan): once nightly. Combination drops simplify routines, which can improve consistency.
Why the Same Times Every Day Matters: Pressure Swings Can Be Harmful
Think of the optic nerve like a delicate wire. If eye pressure is constantly spiking up and down, that repeated stress may contribute to faster glaucoma damage, even if the "average" pressure looks acceptable. Many studies and clinical discussions emphasize that diurnal/nocturnal control and avoiding large swings can matter for long-term outcomes. Research is mixed, and some major studies found that fluctuation was not always an independent risk factor once other variables were considered — but because spikes and gaps in treatment are common in real life, consistent timing remains a practical, important goal in glaucoma care.
Also Consider SLT Therapy
SLT is a laser therapy studied in the LiGHT trial published in 2019 and 2023. It doesn't rely on perfect daily drop use, so real-world control is often better — eye drops only work if they're taken every day, at the right time, with the right technique, and adherence is commonly suboptimal in glaucoma. SLT is a one-visit treatment, so you're not depending on daily dosing, hand strength, memory, or assistance. This is one reason guidelines recommend 360-degree SLT as initial treatment for many newly diagnosed ocular hypertension and open-angle glaucoma patients.
It can keep many patients drop-free for years, with fewer "next-step" treatments. In the LiGHT randomized trial program, SLT-first care was shown to be clinically effective and cost-effective, and long-term follow-up reported that a large proportion of patients remained controlled without drops for years, with reduced need for escalation/surgery compared with drops-first strategies.
It avoids chronic drop side effects, red irritated eyes, and reduced risk of cataract and glaucoma surgery compared to the eye drop group. Many glaucoma drops (especially with long-term exposure to common preservatives like benzalkonium chloride) can worsen dry eye symptoms, irritation, and ocular surface inflammation. SLT lowers pressure without daily chemical exposure on the eye surface, which can be a big quality-of-life win for patients who struggle with redness, burning, or dryness on drops.
Practical Tips to Stay Consistent
Link drops to a daily habit: toothbrushing, coffee, dinner, bedtime. Use phone reminders or a pillbox-style eye drop tracker. If you miss a dose, follow your doctor's guidance — in general, don't "double up" without instructions. Tell your eye doctor if the schedule is hard; often we can simplify with combination drops or once-daily options.
Bottom Line
Glaucoma drops work best when you use the right technique (one drop, eyes closed, inner-corner pressure for 2-3 minutes), and use them at consistent times that match how the medication works and how your eye pressure changes over the day — especially to cover the early-morning pressure rise and reduce harmful pressure swings. </content>